FiledReading9 minViews7
Why 80% of Serious Medical Errors Happen During Patient Handovers
Every 8 hours, in hospitals across Australia, something quietly dangerous happens. Clinical teams change over. A night shift steps in for a day team. An ICU registrar hands their patients to a colleag
Table of contents15 sections

Every 8 hours, in hospitals across Australia, something quietly dangerous happens. Clinical teams change over. A night shift steps in for a day team. An ICU registrar hands their patients to a colleague before heading home after a 10-hour shift. A ward nurse finishes her report and walks to her car.
In those 15 to 30 minutes , sometimes even far less, the entire clinical picture of a patient must be transferred from one human brain to another. Diagnoses, medication changes, deteriorating observations, pending results, allergies, ceilings of care, family conversations, and dozens of other critical details.
And this is where it goes wrong. Consistently. Measurably. Often fatally.
The statistic that gives this article its headline: 80% of serious medical errors involve communication failures, comes from the Joint Commission in the United States, and has been widely replicated in Australian data. But the real picture, when you dig into peer-reviewed research and ACSQHC sentinel event data, is more nuanced, more alarming, and ultimately more actionable than a single number suggests.
This article breaks down the evidence, explains precisely how information gets lost during handover, and explores what Australian hospitals are doing and most importantly what they must do to close the gap.
1. What does "80%" actually mean?
The "80% figure" is one of the most-cited statistics in patient safety literature, but it deserves careful examination. It does not mean that 80% of all handovers produce an error. It means that when serious adverse events are analysed through root cause analysis, communication failure, including handover breakdown, is the contributing factor in the overwhelming majority of cases.
The Australian Commission on Safety and Quality in Health Care (ACSQHC) publishes annual Sentinel Event Review data. Their analysis consistently identifies "communication failures" as the leading system contributing factor in sentinel events: those unexpected events resulting in death or serious patient harm.
"Clinical handover is one of the most vulnerable points in the healthcare system. Information loss during shift changes is not random — it is predictable, patterned, and preventable."
What makes handover particularly risky is its frequency. In a 400-bed Australian hospital, researchers have estimated that over 400 individual patient handover events occur per day , across ward rounds, shift changes, theatre recoveries, inter-hospital transfers and ICU-to-ward step downs. Multiply that by 365 days, and you're looking at hundreds of thousands of risk events per year, in a single hospital.
2. The Science of Why Information Gets Lost
The cognitive science behind handover failure is well-understood, even if the clinical system changes haven't kept pace. Three mechanisms account for the majority of information loss.
Cognitive Load and Working Memory Limits
The human working memory can hold, on average, seven pieces of information (plus or minus two) at a time: a principle established by psychologist George Miller in 1956 and refined extensively since. A typical hospital patient may have 20, 30, or 50 clinically relevant data points at any moment: active medications, pending investigations, advance care directives, infection alerts, fall risk status, and more.
A fatigued junior doctor or nurse at the end of a 10-hour shift is not physiologically equipped to retain and reliably transmit all of this. This is not a failure of individual competence rather, it is a failure of system design.
Interruptions and Environmental Noise
A landmark study published in the Medical Journal of Australia found that the average Australian junior doctor is interrupted 6.6 times per hour during routine clinical work. During handover, which is already a high-cognitive-load task, interruptions are particularly costly. A study of emergency department handovers found that interruptions during handover were significantly associated with omission of clinically important information.
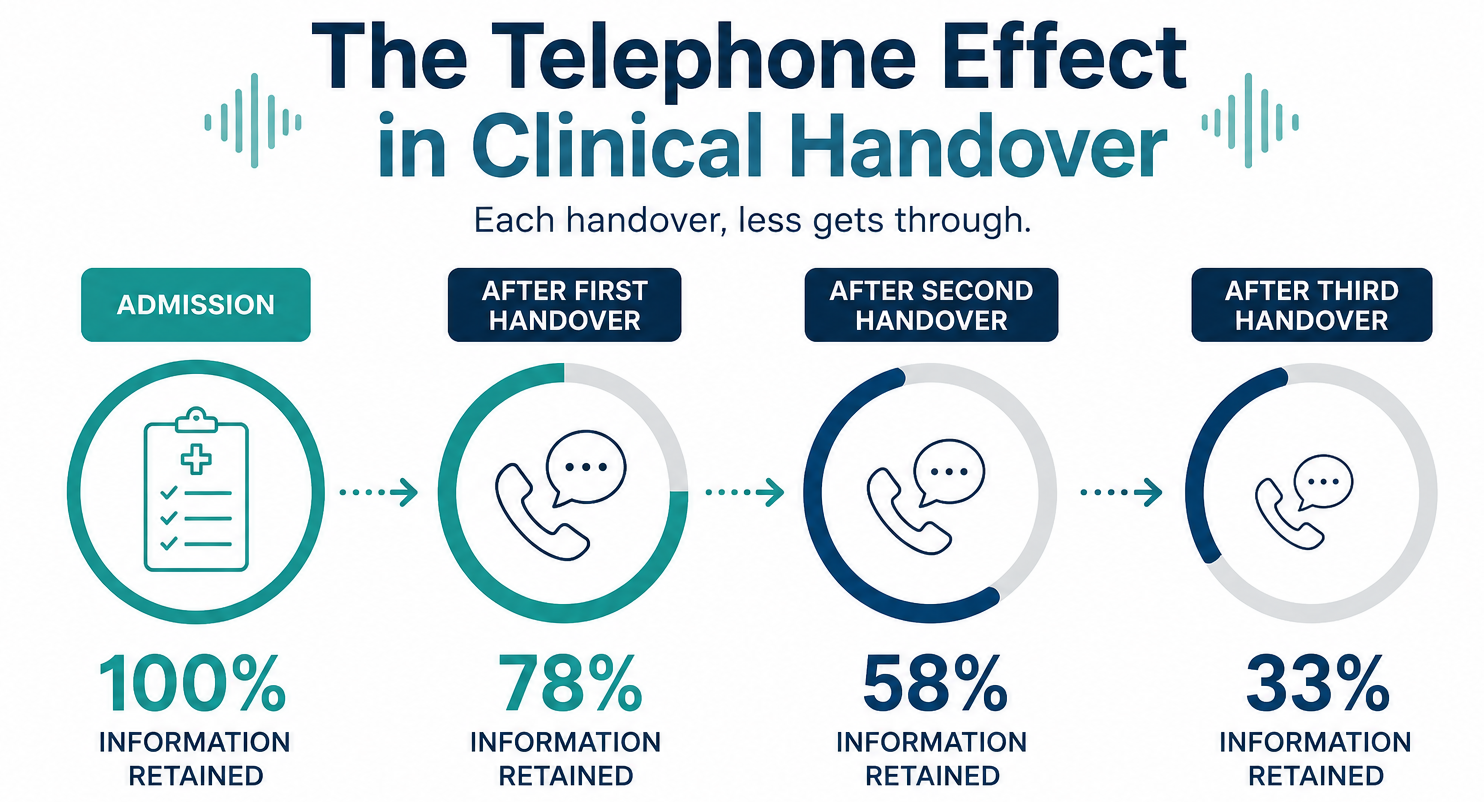
The Telephone Effect: Serial Information Degradation
Bhabra and colleagues demonstrated the "telephone effect" in clinical settings in 2007: when information is passed orally through successive handovers, it degrades exponentially.
After just one handover, approximately one-third of the original information is lost.
After three successive handovers which is just a common over a weekend admission, only a fraction of the original clinical picture survives intact.
The NSQHS Standard 6 Connection NSQHS Standard 6 — Communicating for Safety — directly addresses this risk. Actions 6.07 and 6.08 require hospitals to establish minimum information content requirements for clinical handover and to ensure structured communication tools (such as ISBAR) are consistently used. Non-compliance during accreditation survey is a significant finding.
3. When Handovers Fails: A Risk Timeline
Handover failures rarely produce immediate, visible harm. More often, they create a chain of downstream clinical decisions that are made on incomplete or incorrect information, decisions that compound over hours and days. The following timeline illustrates how a single handover gap can cascade into a serious adverse event.
How a Single Missed Detail Becomes a Sentinel Event
- 1
Day 1 · 07:00 AM
Patient admitted to general medicine with community-acquired pneumonia. Admitting doctor notes penicillin allergy in history. Allergy documented in paper notes but not yet entered into EMR. Patient commenced on appropriate alternative antibiotic.
- 2
Day 1 · 05:00 PM
Afternoon handover occurs — allergy not verbally communicated. The handover is rushed — three patients deteriorated on the ward during the day. The allergy, considered "already managed," is omitted from the verbal handover in favour of more acute information.
- 3
Day 2 · 02:00 AM — ⚠ Risk Point
After-hours JMO reviews patient for worsening fever and low blood pressure. The overnight JMO covering multiple wards has never met this patient. They access the EMR — allergy field is still empty. They escalate to the after-hours registrar who prescribes an antibiotic from the penicillin class.
- 4
Day 2 · 03:30 AM — ⛔ Adverse Event
Patient develops anaphylaxis. Rapid response team activated. Patient transferred to ICU. Length of stay extended by 9 days. Root cause analysis later identifies the original handover omission as the initiating event in the cascade.
This Is Not a Hypothetical Allergy-related medication errors at shift change are among the most frequently reported handover-related adverse events in Australian hospitals. The ACSQHC's "Recognising and Responding to Clinical Deterioration" safety standard directly addresses this cascade. The scenario above reflects the composite pattern documented in multiple published Australian root cause analyses.
4. High-Risk Handover Environments in Australian Hospitals

Not all handovers carry the same risk. Research and ACSQHC data identify specific environments where the probability of information loss is highest.
Emergency Department
The ED presents the perfect conditions for handover failure: high patient volume, undifferentiated presentations, frequent interruptions, and a team structure that changes across multiple overlapping shifts. A systematic review published in Emergency Medicine Australasia found that the ED is the most common site for handover-related adverse events in Australian hospitals.
After-Hours and Night Shift Handovers
After-hours handovers are disproportionately handled by junior doctors who may be covering large numbers of patients they have never met. The "cross-cover" model — where one JMO covers multiple wards overnight — means that handover information must be communicated not just once but across many downstream clinicians. Research consistently shows that clinical deterioration is more likely to go unrecognised during night shifts, and that handover quality is lower when clinicians are fatigued.After-hours handovers are disproportionately handled by junior doctors who may be covering large numbers of patients they have never met. The "cross-cover" model , where one JMO covers multiple wards overnight which means that handover information must be communicated not just once but across many downstream clinicians. Research consistently shows that clinical deterioration is more likely to go unrecognised during night shifts, and that handover quality is lower when clinicians are fatigued.
ICU and Critical Care
ICU patients have the highest information density of any hospital patient — complex medication regimens, ventilator settings, ongoing invasive procedures, family meetings, and minute-by-minute haemodynamic targets. Research shows that ICU handovers routinely exceed the information retention capacity of even experienced clinicians when conducted verbally without structured support.
Inter-Hospital and Ambulance-to-ED Transfers
When patients move between facilities , from a rural hospital to a metropolitan centre, or from an ambulance to an ED, the receiving team is entirely dependent on the information provided by the sending team. There is no access to prior notes. There is no ability to verify what has been said. This is among the highest-risk handover environments identified in Australian patient safety literature.
5. The NSQHS Standard 6 Framework: What Australian Hospitals Must Do
In Australia, the regulatory response to handover risk is codified in NSQHS Standard 6: Communicating for Safety. This standard, which is mandatory for accreditation under both the Australian Council on Healthcare Standards (ACHS) and the NSQHS framework, which sets out specific requirements for how hospitals must manage clinical handover.
| NSQHS Action | What It Requires | Handover-Specific? |
|---|---|---|
| Action 6.07 | Establish minimum information content standards for clinical handover | ✅ Direct |
| Action 6.08 | Implement structured communication tools (e.g. ISBAR) consistently | ✅ Direct |
| Action 6.09 | Ensure patient information is documented and available at all handovers | ✅ Direct |
| Action 6.01 | Establish a clinical governance framework for communicating for safety | Indirect — systemic |
| Action 6.10 | Include patients in clinical handover where appropriate | ✅ Direct |
| Action 6.11 | Audit and evaluate handover performance regularly | ✅ Direct |
Despite these requirements, accreditation surveyors continue to identify handover compliance as one of the most frequently cited areas of improvement across Australian hospitals. The gap between policy and practice remains stubbornly wide — and the consequences continue to accumulate in root cause analyses.
6. What Good Clinical Handover Looks Like
Research on effective handover identifies a consistent set of features that distinguish safe handovers from unsafe ones. These are not difficult to understand but, they are difficult to achieve reliably, at scale, across every ward, every shift, every day.
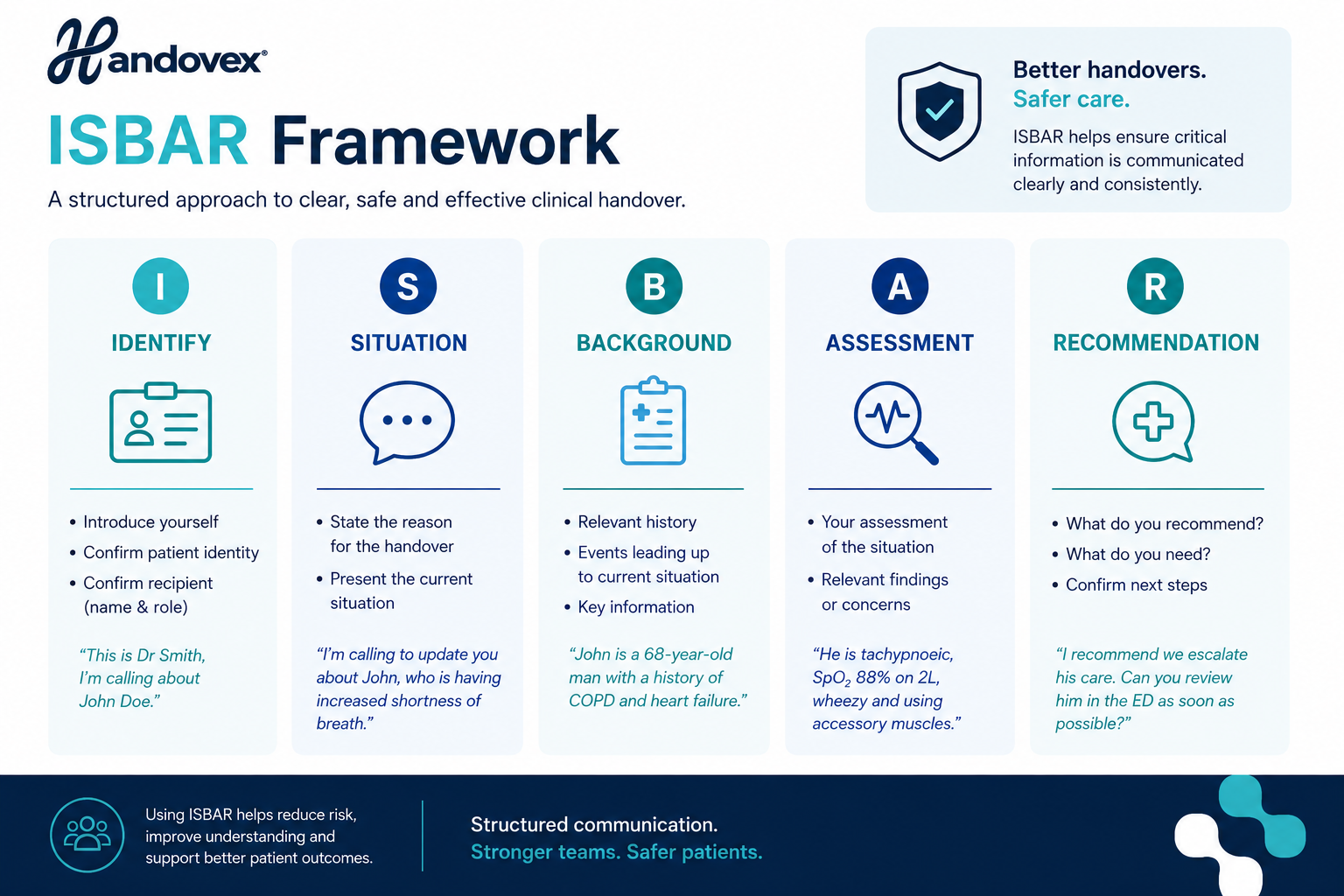
Structured communication, using a framework like ISBAR (Identify, Situation, Background, Assessment, Recommendation) — consistently outperforms unstructured verbal handover in information retention studies. ISBAR is the nationally recommended tool under NSQHS Standard 6 and is the framework mandated in most state health department clinical directives.
Written or documented handover, combined with verbal communication, dramatically reduces information loss. The written record serves as both a cognitive aid during handover and an auditable trail that can be reviewed if questions arise later.
Patient involvement, where appropriate, further improves accuracy. Patients are the only people present at every single handover across their admission — they often remember details that clinicians have omitted or misremembered.
7. How AI Is Changing Clinical Handover
For most of healthcare history, handover improvement initiatives have relied on training, checklists, and culture change: behavioural interventions that require consistent human effort to sustain. The challenge with any behavioural intervention in healthcare is the relentless churn of staff, rostering pressures, and cognitive load that gradually erode compliance.
AI-powered clinical documentation represents a structural shift in how handover safety can be achieved. Rather than relying on a fatigued clinician to remember and accurately communicate 30 pieces of information in 5 minutes, ambient AI systems can listen to verbal handovers in real time, structure the information automatically into ISBAR format, and produce a documented record that is immediately available to the receiving team.
This is not science fiction. Ambient AI scribes, systems that use automatic speech recognition and large language models to produce clinical documentation from verbal conversations, have been deployed in Australian hospital settings and demonstrated measurable reductions in documentation burden. Platforms like Handovex extend this capability specifically to the handover context, with IRAP-certified, ISO 27001-compliant infrastructure built for the Australian healthcare environment.
The Australian Government's Digital Health Strategy, backed by significant investment in 2025–26, explicitly identifies AI-supported clinical documentation as a priority. Hospitals that build this capability now are not just improving safety outcomes — they are positioning themselves ahead of the regulatory and accreditation environment that is rapidly moving in this direction.
See How Handovex Eliminates the Handover Gap
Handovex captures verbal clinical handovers in real time, structures them automatically into ISBAR format, and produces a documented record — without adding a single extra step for your clinical team.
Related posts
The Cost of Failing NSQHS Accreditation — Clinical, Financial, and Reputational
13 May 2026
Most Australian hospital executives focus on the survey itself. Few have fully mapped what non-compliance actually costs — before, during, and after the finding. This guide does exactly that, with dat
The Rise of Ambient AI Scribes in Australian Hospitals: A 2026 Guide to Clinical Documentation
13 May 2026
If you walk into any Australian hospital ward at 6:00 PM, you will likely see the same scene: junior medical officers (JMOs) and senior clinicians huddled around glowing screens, furiously typing. Fo
Related resources
Shareable guides and checklists for safer handovers.
ISBAR best practice
A practical structure for consistent clinical handovers.
Open →NSQHS Standard 6 handover checklist
A lightweight checklist for safer clinical communication.
Open →ISM alignment overview
Auditability, access control, and tenant isolation, at a high level.
Open →