FiledReading5 minViews10
The Cost of Failing NSQHS Accreditation — Clinical, Financial, and Reputational
Most Australian hospital executives focus on the survey itself. Few have fully mapped what non-compliance actually costs — before, during, and after the finding. This guide does exactly that, with dat
Table of contents5 sections
Most Australian hospital executives focus on the survey itself. Few have fully mapped what non-compliance actually costs — before, during, and after the finding. This guide does exactly that, with data.

NSQHS accreditation surveys happen on a cycle. They are predictable. They are announced in advance. And yet, year after year, Australian hospitals receive significant findings — and some receive the most serious outcome of all: conditional or withheld accreditation.
The executives who end up in that position rarely lacked competence. More often, they lacked a clear-eyed view of what accreditation non-compliance actually costs. The full picture, not just the headline finding.
This guide is that picture. It covers the direct financial cost, the extended liability exposure, the reputational damage that is difficult to quantify but impossible to ignore, and critically, which NSQHS standard produces the most frequent significant findings, and why it almost always comes back to clinical handover.
35%
#1
4.1
1.What NSQHS Accreditation Actually Tests
The NSQHS (National Safety and Quality Health Service) Standards are administered by the Australian Commission on Safety and Quality in Health Care and define the minimum level of care Australian hospitals and health services must provide. There are eight standards in the current framework. Accreditation is not optional: public hospitals are required to be accredited, and private hospitals require accreditation for health fund contracting.
Surveyors assess hospitals against specific "actions" within each standard. Findings are graded:
1. Met
2. Not Met — Recommendation
3. Not Met — Significant Finding
4. Conditional Accreditation
Conditional Accreditation Has Operational Consequences Beyond the Finding Itself A conditionally accredited hospital faces mandatory reporting obligations to state health departments, potential limitations on service delivery (particularly elective procedures), impact on private health fund agreements, and reputational damage that directly affects patient volumes and medical workforce retention. These consequences compound over time if remediation is slow.
2. Why Standard 6 Is the Most Frequent Finding
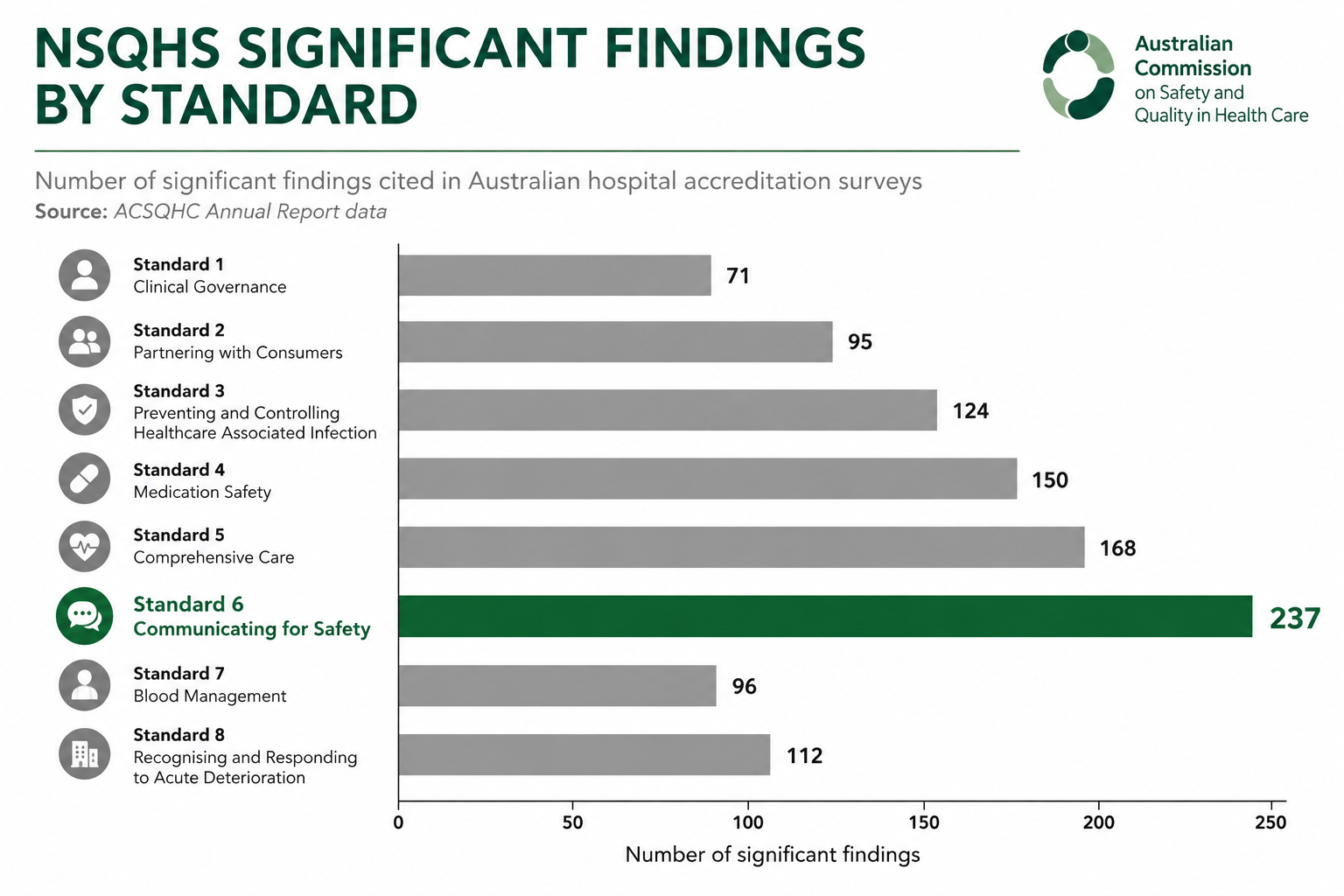
Standard 6 — Communicating for Safety — requires hospitals to demonstrate that they have established and consistently operate a system for safe clinical communication, including clinical handover. This sounds straightforward. In practice, it is the area where the gap between policy and real-world implementation is most visible to surveyors.
Surveyors don't just review policies. They speak to nurses, doctors, and allied health staff. They observe handovers. They review medical records and look for documentation patterns. They ask staff if they know what ISBAR is, whether they use it, and whether they feel safe raising concerns about clinical communication failures.
A hospital can have a beautifully written clinical handover policy and still receive a significant finding under Standard 6, because the surveyor's job is to determine whether that policy is being enacted in practice — by a night-shift nurse at 3am, by a JMO covering three wards after-hours, by a surgical ward nurse at the weekend. Policy compliance is not the same as practice compliance.
The specific actions under Standard 6 that most frequently generate significant findings are Actions 6.07, 6.08, 6.09, and 6.11 — covering minimum information content at handover, use of structured communication tools, documentation of handover, and audit of handover quality respectively. These four actions describe a system that should be working every day, on every ward, at every shift change. Demonstrating that it does requires more than a folder of audits.
3. The Full Financial Cost: A Line-by-Line Breakdown
Hospital boards often see accreditation preparation as a compliance exercise with a known budget. The real cost exposure is considerably broader. The following breakdown categorises the costs that NSQHS non-compliance generates — distinguishing between preparatory costs (which are incurred by every hospital, compliant or not), remediation costs (incurred after a finding), and downstream liability exposure.
For Comparison: The Cost of Prevention A technology-enabled clinical handover improvement program — including AI documentation support, staff training, and audit tooling — typically costs between $80,000 and $350,000 for a 400-bed hospital in the first year. The ROI case, viewed against even the most conservative estimate of adverse event and remediation costs, is not marginal. It is structural.
4. The Reputational Risk That Doesn't Show Up in the Budget
Australian hospital accreditation findings are public documents. The NSQHS framework requires that survey outcomes — including significant findings — are reported to health departments and made available through public reporting mechanisms. For private hospitals, accreditation status is visible to health funds. For public hospitals, findings become subject to Freedom of Information requests, ministerial briefing processes, and, increasingly, media reporting.
The reputational consequences of a public significant finding under Standard 6 are difficult to model financially, but experienced hospital executives describe a consistent pattern:

5. The Executive Decision: Accreditation as Strategy, Not Compliance
The executives who navigate NSQHS accreditation most successfully are those who have reframed the question. They are not asking "how do we pass the survey?" They are asking "what does genuinely safe clinical communication look like in our hospital, and how do we build the infrastructure to sustain it — independent of the survey cycle?"
That reframing has a practical implication: the interventions that produce durable NSQHS Standard 6 compliance are the same interventions that reduce adverse event rates, reduce medicolegal exposure, improve clinical staff satisfaction, and reduce documentation burden. They are not separate programs. They are one investment with multiple returns.
AI-supported clinical handover documentation — systems that automatically structure and record verbal handovers in real time, without adding steps for clinical staff — is increasingly the infrastructure choice of hospitals that want to achieve this. Not because technology replaces the need for clinical communication culture, but because it removes the structural barriers that prevent that culture from sustaining itself under the pressure of shift work, fatigue, and competing clinical demands.
Handovex is built specifically for this purpose, in the Australian healthcare context, with IRAP-assessed security infrastructure and native support for NSQHS Standard 6 documentation requirements.
Related posts
The Rise of Ambient AI Scribes in Australian Hospitals: A 2026 Guide to Clinical Documentation
13 May 2026
If you walk into any Australian hospital ward at 6:00 PM, you will likely see the same scene: junior medical officers (JMOs) and senior clinicians huddled around glowing screens, furiously typing. Fo
Why 80% of Serious Medical Errors Happen During Patient Handovers
8 May 2026
Every 8 hours, in hospitals across Australia, something quietly dangerous happens. Clinical teams change over. A night shift steps in for a day team. An ICU registrar hands their patients to a colleag
Related resources
Shareable guides and checklists for safer handovers.
ISBAR best practice
A practical structure for consistent clinical handovers.
Open →NSQHS Standard 6 handover checklist
A lightweight checklist for safer clinical communication.
Open →ISM alignment overview
Auditability, access control, and tenant isolation, at a high level.
Open →